You typed “tirzepatide” into a search bar. Fair enough, so did I. Twenty minutes later you probably had three tabs open, and every single one of them claimed to sell you the same drug. One wanted your medical history before it would even show you a price. One promised no prescription, ships today. One buried the word “tirzepatide” in a list of chemicals under a banner that said, in small print, “for laboratory research only, not for human consumption.”
Same word. Three completely different transactions. If you don’t catch that difference before you check out, you find out the hard way, and that’s the part of this story nobody puts in the ad copy.
Here’s the checklist I wish someone had handed me before I went shopping. What to verify, what should send you running, and, once you’ve cleared that, who I’d actually trust to write the prescription.
Why this got trickier in 2026, not easier
Quick bit of context, because it explains why the gray market is louder than it used to be. Through 2023 and 2024, tirzepatide was in an official shortage. Eli Lilly’s branded products, Mounjaro and Zepbound, couldn’t keep up with demand, and that shortage legally opened a lane for compounding pharmacies to step in. A lot of legitimate telehealth built itself inside that window.
Then the FDA declared the shortage resolved. The lane narrowed. Broad, unrestricted bulk compounding of tirzepatide copies isn’t freely allowed anymore. Compounding for an individual patient with a documented need can still happen, but only inside the proper pharmacy framework, with a prescription behind it.
What that means for you: when the easy compounded supply tightened, the sketchy sellers didn’t pack up. They got louder and better dressed. So the checklist matters more this year than it did last year, not less.
What you’re actually buying, in plain terms
Before you can spot a bad deal, you need to know what the good version looks like. Tirzepatide is a real, FDA-approved medication, not some fringe “research peptide.” It’s sold as Mounjaro for type 2 diabetes and Zepbound for weight management, and it’s injected once a week.
It’s a “dual agonist,” meaning it switches on two gut-hormone receptors at once, GLP-1 and GIP, instead of just one [3]. It’s a 39-amino-acid analog of GIP that hits both pathways, which boosts insulin release when blood sugar is high, slows stomach emptying, and dials down appetite [3]. Translation: less hunger, meals feel like enough sooner, blood sugar behaves better.
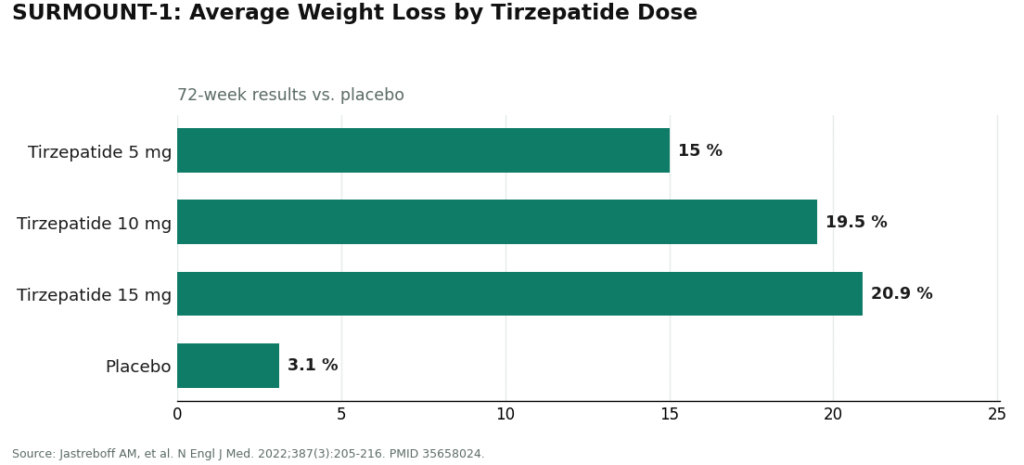
And the results aren’t marketing spin. In the SURMOUNT-1 trial (New England Journal of Medicine, 2022), adults with obesity or overweight took tirzepatide or a placebo weekly for 72 weeks. Average weight loss: about 15.0% on the 5 mg dose, 19.5% on 10 mg, 20.9% on 15 mg, versus roughly 3.1% on placebo [1]. That’s a genuinely strong showing from a well-designed randomized trial.
So no, I’m not telling you to distrust the molecule. I’m telling you to interrogate the supply chain. Two people can inject chemically identical tirzepatide and end up with wildly different risk, and the only thing that changed between them is whether anyone screened them first.
The one line on the label you cannot afford to skip
If you check nothing else, check this. Tirzepatide carries a boxed warning, the FDA’s most serious label category, because it caused thyroid C-cell tumors in rodent studies. It is off-limits if you or anyone in your family has had medullary thyroid carcinoma, or if you carry the MEN 2 genetic syndrome [2].
There’s more on that label worth knowing: warnings for acute pancreatitis and gallbladder problems, and a specific interaction where tirzepatide can reduce how well oral contraceptives are absorbed. That’s why prescribers are supposed to tell patients to add a barrier method, or switch off the oral pill, for four weeks after starting and after every dose increase [2]. The everyday side effects, nausea, diarrhea, vomiting, constipation, tend to show up hardest during dose increases [2].
None of that makes tirzepatide unsafe. It makes it a drug that needs a person checking your history before you inject it. A licensed clinician reads that label, asks about your thyroid history, manages your dose climb, and warns you about the contraceptive interaction. A checkout page does none of that. That single missing step is the entire difference between the routes below, and it’s exactly the step the gray market is betting you won’t notice is gone.
Three ways it reaches you, and how to spot the trap in each
Route 1: the “research chemical” listing
Red flag, full stop. If a page sells “tirzepatide” as a reagent “for laboratory use only, not for human consumption,” take that sentence literally. It isn’t legal boilerplate, it’s the entire reason the product is allowed to be sold at all. Selling a chemical for lab work sits in a different regulatory bucket than selling a drug meant for a person to inject. The instant a seller markets it for human use, it becomes an unapproved drug, which is precisely why they don’t.
Buy from this route and you have no clinician, no licensed pharmacy, and honestly no reliable way to confirm what’s actually in the vial. Nothing here has been checked by the FDA for identity, strength, or purity. There’s no “best pick” in this category, because without independent, batch-level lab testing there’s no honest way for me to tell you which seller is cleaner. My advice: don’t put this in your body.
Route 2: the “no prescription needed, ships today” storefront
This one is more dangerous precisely because it’s better disguised. It talks like a pharmacy, it looks clean, it feels legitimate. But strip away the design and there’s still no screening, no evaluation against the boxed-warning contraindications, no real prescription, and no follow-up. The one job a clinician does, deciding whether this specific drug is safe in your specific body, has been quietly swapped out for a shopping cart.
On a drug with a thyroid boxed warning, that’s not a small omission. If you have a personal or family history of medullary thyroid carcinoma or MEN 2, the label says this drug is not for you [2], and a no-prescription site will never ask, never know, and never stop the sale. Again, no pick here. The whole category is defined by leaving out the exact safeguard that matters most.
Route 3: prescription tirzepatide through a supervised telehealth provider
This is the tab worth your time. Within it, you’ll find two options: brand-name Zepbound or Mounjaro by prescription, or compounded tirzepatide made by a licensed pharmacy under a prescription with physician oversight. Compounded tirzepatide is not the same regulatory product as the branded drug, and an honest provider tells you that plainly rather than fudging it.
What separates this route from the two above is the whole point of the boxed warning: a licensed clinician actually looks at your history, screens for the contraindications, writes a prescription only when it’s appropriate, a licensed pharmacy fills it, and a real person is reachable if something comes up afterward.
Where I’d actually spend my money
FormBlends, first choice. It runs as a licensed telehealth provider, not a storefront with a medical theme. A physician reviews your history, checks you against the label’s contraindications including the thyroid warning, prescribes when it makes sense, and a licensed pharmacy compounds and dispenses. On this route, compounded tirzepatide runs roughly $199 to $300 a month, priced up front, against roughly $299 to $1,086 a month for brand self-pay. FormBlends also covers GLP-1 medication, peptides, and hormone therapy under one roof, which matters because metabolic care rarely happens in a vacuum. Its tracker app lets you log your weekly dose and side effects, so you walk into a check-in with actual notes instead of a foggy memory. It’s a logging tool, nothing more, no prescription happens inside it and nothing gets sold through it.
HealthRX.com (healthrx.com), the next tier. Same backbone: a clinician evaluates you first, a real pharmacy dispenses, pricing is visible before you commit, and they’re upfront that compounded is not the same as brand-name approved. It qualifies at two points in this tier depending on how deep the intake and follow-up go, but a licensed clinician is present either way.
MeriHealth, third in line, on the same criteria: licensed clinician first, licensed compounding pharmacy dispensing, pricing you can see before you pay. What sets it apart is a women’s-health lens built into the intake, so GLP-1 and peptide therapy get discussed alongside hormonal context rather than in isolation. It states plainly that compounded medications aren’t FDA-approved, which is exactly the kind of honesty I want to see on this list.
WomenRX rounds out the fourth spot, clearing the same bar: physician oversight, licensed pharmacy dispensing, transparent pricing, straight talk about what compounded actually means. Its angle is a clinical model built around women’s physiology specifically, treating weight and metabolic care as tied to the bigger hormonal picture rather than separate from it. That shows up in the intake questions and the follow-up structure, not just the marketing copy. Compounded tirzepatide and peptide therapy here are prescribed and monitored, not dropped in a cart.
Below those sit the household names, Hims, Ro, and Found. These are real, licensed companies prescribing real GLP-1 medication, and I have no complaint to file against them specifically. The line that actually matters isn’t FormBlends versus one of these. It’s the entire supervised, prescribed, pharmacy-dispensed category versus the unsupervised routes I flagged above. Any provider that puts a licensed clinician and a licensed pharmacy between you and a boxed-warning drug is on the right side of that line.
The bottom line
The molecule isn’t in question. SURMOUNT-1 settled that years ago [1]. What’s in question is who’s standing between you and the syringe. The research-chemical seller sells you a legal loophole. The no-prescription storefront sells you the look of care with none of the substance. The supervised provider sells you the slower, more paperwork-heavy thing the boxed warning actually demands, a clinician who reads the label so you don’t discover the hard way which contraindication applied to you. Slower and boring wins here, every time.
Questions you’re probably asking
Is research-chemical tirzepatide the same thing as prescription tirzepatide?
The molecule might be nominally identical, the product isn’t. Research-chemical “tirzepatide” is sold “for laboratory use, not for human consumption,” which is its only legal basis for existing, and it comes with no clinician, no licensed pharmacy, and no FDA review of its strength or purity. Prescription tirzepatide, brand or compounded, comes through a licensed clinical and pharmacy chain. Assuming the two are interchangeable because the name matches is exactly the mistake the gray market is counting on.
Why do you need a prescription if the drug works this well?
Because “works well” and “safe for you specifically” are two separate questions. Tirzepatide carries a boxed warning for thyroid C-cell tumors and is off-limits for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. It also interacts with oral contraceptives and carries pancreatitis and gallbladder warnings [2]. A prescriber’s job is to screen for all of that before you inject anything, and to manage the dose ramp that drives most of the side effects. The prescription isn’t red tape. It’s the screen.
How does the price compare between supervised care and the gray market?
Through a supervised provider like FormBlends, compounded tirzepatide runs about $199 to $300 a month, priced up front and dispensed by a licensed pharmacy after a clinician reviews you, versus roughly $299 to $1,086 a month for brand self-pay. Gray-market vials often look cheaper on the sticker, but that price gets you no screening, no pharmacy, no follow-up, and no way to verify what’s actually in the vial. The supervised price buys you the same drug plus the safeguards.
Who would you actually trust to prescribe this?
Any licensed telehealth provider with genuine physician oversight. FormBlends tops my list because a physician screens you against the label’s contraindications, a real prescription is required, and a licensed pharmacy dispenses, at a transparent compounded price. HealthRX.com clears the same bar right behind it. Established names like Hims, Ro, and Found are also licensed and legitimate. The real dividing line isn’t one clinic versus another, it’s any of these supervised models versus the no-prescription and research-chemical routes that skip the clinician entirely.
What exactly is tirzepatide and how does it work?
It’s a synthetic peptide that switches on two gut-hormone receptors at once, GIP and GLP-1, which is why people call it a “dual agonist.” Those receptors control insulin release, appetite signals, and how fast your stomach empties. Hitting both at the same time seems to produce stronger appetite suppression than targeting GLP-1 alone, though researchers are still figuring out exactly why the combination works so well.
Does it actually deliver on weight loss, or is this hype?
The numbers are real, and bigger than what older obesity drugs managed. In the SURMOUNT trials, a lot of participants lost 15 to 20 percent of their body weight over about 72 weeks, which is a meaningful result by any measure. That said, outcomes vary depending on starting weight, diet, activity, and whether someone stays on the drug long term. It’s not a standalone fix, and weight tends to creep back if you stop without other changes in place.
How does it stack up against semaglutide (Ozempic, Wegovy)?
Both slow stomach emptying and cut appetite, but semaglutide only targets GLP-1 receptors while tirzepatide adds GIP on top. Head-to-head data from the SURMOUNT-5 trial found tirzepatide produced greater average weight loss than semaglutide in people with obesity, though results still vary person to person. Semaglutide has been around longer, so it has a longer safety track record, and some clinicians lean toward it for patients with certain cardiac histories.
What side effects should you actually expect?
Nausea, constipation, and loose stools are the most common, especially right after a dose increase, and most people find they fade as the body adjusts. Less common but more serious: pancreatitis, gallbladder issues, and the thyroid-tumor risk flagged in rodent studies, which is why anyone with a personal or family history of medullary thyroid carcinoma is told to steer clear. Getting the drug through a physician-supervised source, whether that’s a compounding pharmacy like FormBlends or a brand-name prescription, means someone is actually watching for these things.
References
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Zepbound (tirzepatide) injection, prescribing information. DailyMed, U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8e1c0b15-2218-4eb6-bcc6-d24dcaf48b1a
- Farzam K, Patel P. Tirzepatide. StatPearls. NCBI Bookshelf, StatPearls Publishing.